Addison’s Disease: Symptoms, Crisis Warning Signs, and Recovery Strategies
Overview of Addison’s Disease
Addison’s disease (primary adrenal insufficiency) is a rare but serious condition in which the adrenal glands do not produce enough cortisol and often aldosteroneendocrinologyadvisor.com. Cortisol is vital for stress response, blood pressure maintenance, and metabolism, while aldosterone helps regulate salt and water balancemy.clevelandclinic.orgmy.clevelandclinic.org. Addison’s disease is most commonly caused by an autoimmune destruction of the adrenal cortex (especially in women)endocrinologyadvisor.comendocrinologyadvisor.com, though it can also result from infections (like tuberculosis or fungal infections), adrenal bleeding, or metastatic cancerniddk.nih.govendocrinologyadvisor.com. The condition can affect adults of any age and sex, but often presents between 30–50 years old and has a slight predilection for females due to autoimmunityendocrinologyadvisor.commy.clevelandclinic.org. Addison’s is chronic and progressive: symptoms typically develop slowly over months or years and are often vague, which is why the diagnosis is frequently delayed or overlooked until an emergency (adrenal crisis) occursniddk.nih.govendocrinologyadvisor.com.
Comprehensive Symptoms of Addison’s Disease
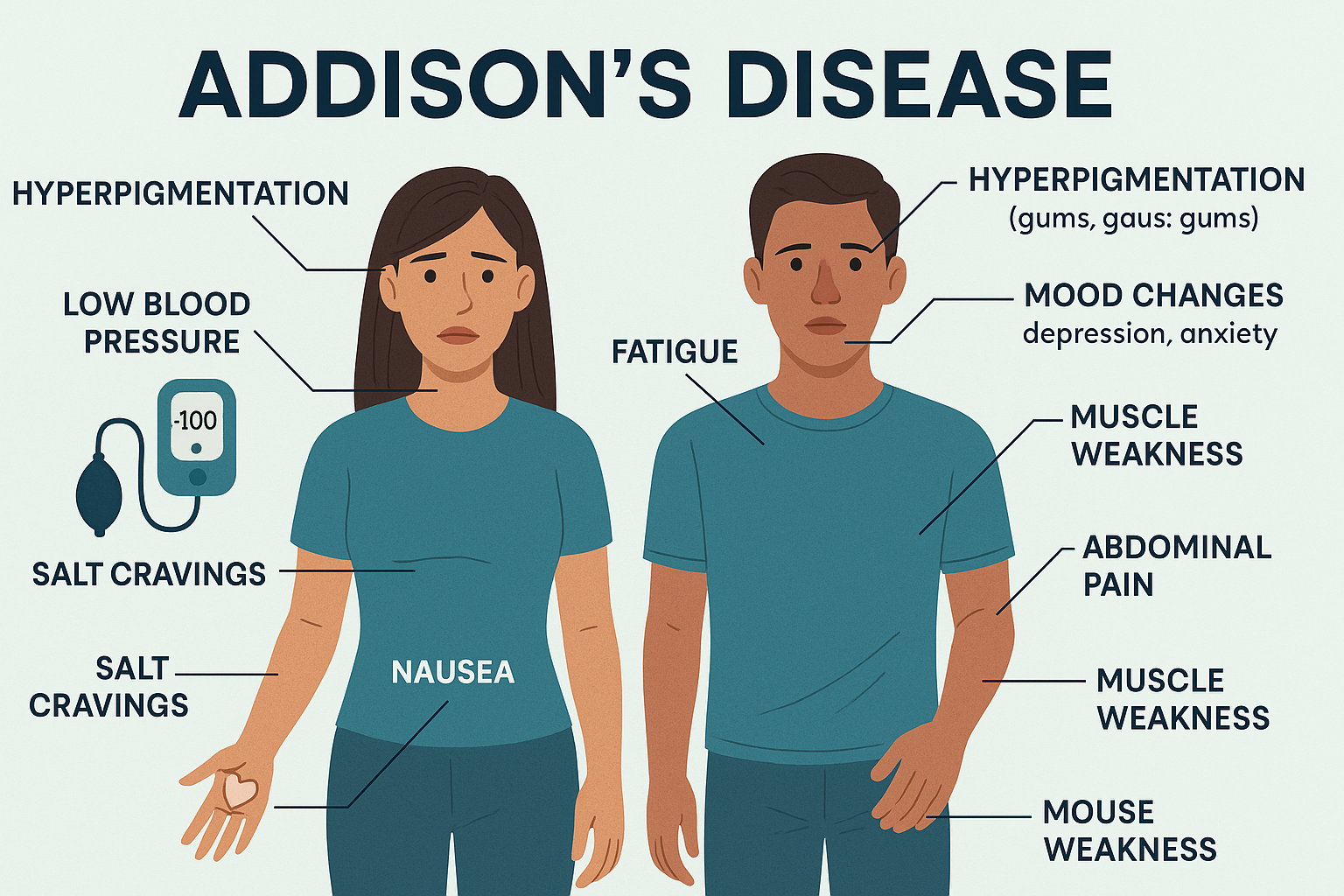
Common symptoms: Addison’s disease usually causes a constellation of nonspecific symptoms that gradually worsen. Key symptoms and signs include:
- Chronic fatigue and muscle weakness: Profound, long-lasting fatigue (often the most common complaint) and generalized weakness are hallmark symptomsniddk.nih.govmy.clevelandclinic.org. Patients often feel exhausted even with adequate rest.
- Loss of appetite and weight loss: Many develop anorexia (loss of appetite) and unintentional weight loss over timeniddk.nih.govaafp.org. In fact, nearly all untreated patients experience some degree of weight loss and anorexiaaafp.org.
- Gastrointestinal issues: Nausea, recurrent vomiting, abdominal pain, and sometimes diarrhea are frequentniddk.nih.govmy.clevelandclinic.org. Some patients also report constipation on occasionendocrinologyadvisor.com (possibly from dehydration). These GI symptoms contribute to poor appetite and weight loss.
- Skin hyperpigmentation: Darkening of the skin (melanin pigmentation) is a classic sign in primary Addison’s. This “bronzing” or muddy complexion often appears in skin folds, creases of the palms, knuckles, knees, elbows, scars, lips, and even inside the cheeks (buccal mucosa)niddk.nih.govendocrinologyadvisor.com. It can look like an inexplicable tan or patches of dark skin. Note: This occurs in ~90% of primary Addison’s cases due to high ACTH levels stimulating melaninaafp.org, but it may be subtle or absent in some patients (especially in secondary adrenal insufficiency or in very fair-skinned individuals)onlinelibrary.wiley.com.
- Low blood pressure (hypotension): Blood pressure is typically low, and orthostatic hypotension (feeling dizzy or faint when standing up) is commonniddk.nih.govaafp.org. Systolic blood pressure <110 mmHg is noted in ~90% of patientsaafp.org. This can manifest as lightheadedness, “seeing stars,” or even fainting episodes in severe cases.
- Electrolyte disturbances: Due to aldosterone deficiency, patients often have low sodium and high potassium. This can cause salt cravings (a strong urge to eat salty foods)niddk.nih.gov and can contribute to dehydration. About 16% of patients report salt-craving behavioraafp.org, which is an important clue if present. High potassium can lead to muscle cramps or palpitations, though these symptoms are less obvious and usually detected via lab tests.
- Dehydration: Patients may show signs of dehydration (due to both aldosterone-related salt loss and vomiting). They might have dry mucous membranes or feel very thirsty. Chronic dehydration can further lower blood pressure and cause dizzinessmy.clevelandclinic.orgmy.clevelandclinic.org.
- Muscle and joint pain: Achy muscles, joint pains, or unexplained chronic pain can occurendocrinologyadvisor.commy.clevelandclinic.org. These aches are often diffuse. Some patients experience muscle spasms as wellmy.clevelandclinic.org, likely related to electrolyte imbalances (low sodium).
- Hypoglycemia episodes: Cortisol helps maintain normal blood sugar, so its deficiency can lead to low blood glucose (hypoglycemia), especially in times of fasting or exertionniddk.nih.gov. This may cause shakiness, sweating, intense hunger, or confusion – symptoms that can be mistaken for other disorders.
- Neuropsychiatric symptoms: Addison’s often affects mood and mental state. Irritability, low mood or depression, anxiety, and lack of motivation are frequently reportedniddk.nih.govmy.clevelandclinic.org. Patients might appear apathetic or have difficulty concentrating. In some cases, mild cognitive impairment (brain fog) or memory issues occur due to chronic low cortisol and low sodium. Family might notice the person is more withdrawn or unusually down.
- General weakness and “failure to thrive”: Especially in older adults, Addison’s can present as an overall functional decline – severe fatigue, weakness getting worse, and inability to carry out normal activitiesagsjournals.onlinelibrary.wiley.comagsjournals.onlinelibrary.wiley.com. For a 60-year-old woman, this might initially be mistaken for “just aging” or another chronic illness if clinicians are not vigilant.
Often-overlooked signs: Because many symptoms are nonspecific, certain subtle signs of Addison’s disease are easily missed or attributed to other causesendocrinologyadvisor.comaafp.org. Here are a few that warrant attention:
- Skin changes in hidden areas: While hyperpigmentation on sun-exposed skin can be obvious, look for it in less noticed areas – e.g. the gums and inner cheeks (which may show a bluish-black discoloration), new scars turning dark, or knuckles and nail beds becoming more pigmentedniddk.nih.govccjm.org. Hyperpigmentation can be subtle initially, and patients or doctors might overlook a “slight tan” – especially if it’s winter or the person is not sunbathing (a tan without sun exposure is a red flag). Conversely, about 10–20% of autoimmune Addison’s patients may develop vitiligo (white patchy depigmentation)aafp.org, an autoimmune skin condition; seeing vitiligo alongside fatigue and hyperpigmented scars should raise suspicion.
- Salt cravings and low blood sodium: Craving very salty snacks or even adding extra salt to meals can be an overlooked symptom – patients might not mention it unless asked. Hyponatremia (low sodium) can also cause headaches, mild confusion, or even an altered sense of taste, which might be written off as something else.
- Orthostatic dizziness or “wobbly knees”: Feeling unsteady or having “wobbly” legs when standing due to drops in blood pressure is a subtle clue of adrenal insufficiency. Patients might just say they feel dizzy when they get up, or that their knees feel weak – this can easily be attributed to dehydration or aging. Being attuned to this symptom is important as it suggests cortisol/aldosterone deficiency affecting circulationniddk.nih.gov. Addison’s patient advocacy groups advise being alert to signs like unusual headaches, stomach aches, or knee bucklingwhen one’s steroid is wearing off, as these can herald an impending crisis if not addressed (e.g. time for a dose or need for stress dose)scribd.com.
- Mood and personality changes: A subtle apathy, loss of interest in hobbies, or unusual irritability may develop slowly. Because these changes are gradual, family and even healthcare providers might label it as depression, stress, or “just getting older.” In reality, low cortisol can significantly affect neuropsychiatric stateniddk.nih.gov. If someone has new-onset depression or anxiety along with physical symptoms like weight loss or skin changes, Addison’s should be considered.
- Loss of axillary/puberty hair and sexual changes: In women, adrenal androgen loss can cause thinning of body hair (especially underarm and pubic hair) and low libidoniddk.nih.govmy.clevelandclinic.org. Post-menopausal women (like a 60-year-old) might not notice the hair loss as much, or it may be attributed to aging, but it can be a clue if other signs are present. Men with Addison’s may experience some loss of libido or energy, but because men produce testosterone from their testes, they usually don’t notice hormone-related sexual changes as dramatically as women do.
- Frequent infections or slow recovery: Cortisol is important for immune response, so some Addison’s patients report they become more prone to infections or take longer to recover from illnesses. While not a classic textbook symptom, recurrent infections or an inability to bounce back from a mild illness could be an overlooked hint, especially in an older adult whose immune function might already be weaker.
Clinical tip: Addison’s disease symptoms are often mistaken for other conditions (gastrointestinal disorders, depression, chronic fatigue syndrome, etc.). In fact, one study found patients often saw multiple providers over months/years before diagnosispulsetoday.co.uk. If someone “just doesn’t feel right” for a long time – with fatigue, weight loss, or skin changes – it’s worth testing adrenal function. Early treatment of Addison’s can prevent a life-threatening crisisniddk.nih.gov.
Example of hyperpigmentation in Addison’s disease. In primary Addison’s, excess ACTH can cause diffuse tanning or dark patches. Left: A patient’s hands showing markedly darkened skin in the creases and knuckles. Right: A normal skin tone for comparison. Hyperpigmentation like this, especially if appearing without sun exposure, is a key sign of Addison’s diseaseemedicinehealth.com. (Not all cases are this obvious – early changes may be subtle or mistaken for a regular tan.)
Early Warning Signs of an Addisonian Crisis and How to Prevent One
What is an Addisonian crisis? An Addisonian crisis (adrenal crisis) is an acute, life-threatening exacerbation of adrenal insufficiency. Essentially, the body’s cortisol level becomes critically low relative to need, leading to shock(very low blood pressure and organ hypoperfusion) along with dangerous electrolyte imbalancesncbi.nlm.nih.govncbi.nlm.nih.gov. This is a medical emergency that can be fatal if not treated promptly with high-dose corticosteroids and supportive carencbi.nlm.nih.govncbi.nlm.nih.gov. Crises often occur in people with known Addison’s disease during a severe stress (e.g. infection), but in about half of cases, an adrenal crisis is the first presentation of undiagnosed Addison’s diseasencbi.nlm.nih.govncbi.nlm.nih.gov.
Early warning signs of an impending crisis: It’s crucial for patients and caregivers to recognize the early signs that cortisol levels are dropping to dangerously low levels. Initial symptoms of an adrenal crisis can mimic a bad flu or gastroenteritis, and they can escalate rapidly. Watch for:
- Severe weakness and fatigue: Beyond the chronic tiredness of Addison’s, a crisis often starts with an extreme, sudden worsening of weakness. Patients may feel unable to stand (“legs giving out”) or profoundly exhausted to the point of near-collapsemy.clevelandclinic.orgmy.clevelandclinic.org. This often comes on quickly (over hours to a day).
- Dizziness and drop in blood pressure: If standing up causes immediate faintness, or if the person feels light-headed even lying down, it indicates worsening hypotension. Syncope (fainting/passing out) is a serious warning signendocrinologyadvisor.commy.clevelandclinic.org. Many patients describe a unique kind of dizziness or a “feeling of doom” as their blood pressure plummets. Family might notice the person looks pale and unsteady.
- Abdominal pain, nausea, and vomiting: Intense stomach pain (sometimes spreading to the lower back or legs) can occur at the start of a crisismy.clevelandclinic.org. This may be accompanied by cramping, nausea, and repeated vomitingmy.clevelandclinic.orgmy.clevelandclinic.org. If an Addisonian patient suddenly cannot keep down their oral steroids due to vomiting, an adrenal crisis can develop very fast – this is an emergency situation.
- Diarrhea: Profuse diarrhea often joins vomiting in a crisis, worsening dehydration and salt lossnhs.ukmy.clevelandclinic.org. The combination of vomiting and diarrhea in an Addison’s patient is particularly dangerous, as it means they’re losing fluid and cannot absorb oral medication.
- Headache and confusion: An emerging crisis may cause a severe headache, along with confusion, restlessness, or an anxious “panicky” feelingmy.clevelandclinic.orgnhs.uk. Loved ones might notice the patient becoming disoriented, unusually irritable or even combative as their brain gets less perfusion and hypoglycemia sets in. Agitation or feeling intensely fearful for no obvious reason can be an early neuropsychiatric red flag of impending adrenal crisismy.clevelandclinic.org.
- Fever or chills: Sometimes a fever is the trigger (if an infection precipitated the crisis) and the patient may look ill with sweating or cold, clammy skinnhs.ukmy.clevelandclinic.org. Even without infection, low cortisol can impair temperature regulation, so mild fever can occur, or conversely the person may have a lower than normal body temp and cold sweat.
- Signs of shock: As crisis progresses, signs of shock appear: pale, clammy skin, a rapid but weak pulse, and rapid shallow breathingnhs.ukmy.clevelandclinic.org. The patient may complain their heart is pounding (tachycardia) or may start breathing fast due to acidosis. Severe drowsiness or loss of consciousness is an extremely grave sign – indicating the brain isn’t getting enough blood sugar or pressurenhs.uk. This is late in a crisis; ideally, treatment begins long before this point.
In summary: If a person with Addison’s disease experiences unusual fatigue, dizziness, abdominal pain, and vomiting – especially all at once – assume it’s an adrenal crisis until proven otherwise and take action. Caregivers should also trust their instinct; many Addison’s patients describe a distinctive “I am about to crash” feeling.
Preventing a crisis: The good news is that with vigilant management, many adrenal crises are preventable. Key prevention strategies include:
- Never skip your steroid medication: Missing doses of hydrocortisone, prednisone, or fludrocortisone can precipitate a crisisnhs.uk. Take medications exactly as prescribed every day and ensure you have refills. For a 60-year-old woman with possible memory issues, using alarms or pill boxes can help avoid missed doses.
- “Sick day” rules (stress dosing): Work closely with your endocrinologist on how to adjust your steroid dose during illnesses or stressnhs.ukncbi.nlm.nih.gov. As a rule of thumb, if you have a fever, severe illness, or injury, you will need a higher dose of corticosteroid. For a mild illness (like a common cold with no fever), doubling the daily glucocorticoid dose for a couple of days is often recommended; for more severe stress (high fever >101°F, significant injury, surgery, etc.), doses may need to be 2–3 times higher or an injection may be neededncbi.nlm.nih.gov. This proactive increase (“stress dosing”) supplies your body the extra cortisol it would normally produce in stress, and it can avert a crisis. Never tough out a serious illness on normal Addison’s doses – always seek medical advice about increasing steroidsnhs.uknhs.uk.
- Keep an emergency hydrocortisone injection kit: All adrenal insufficiency patients should have an emergency glucocorticoid injection available (e.g. hydrocortisone or dexamethasone vial)nhs.uk. You and a close family member should be trained on intramuscular injection techniquenhs.uk. At the first sign of an impending crisis (e.g. inability to keep pills down due to vomiting, or symptoms like severe weakness and confusion), administer the emergency injection immediately – don’t wait until collapse occursnhs.uk. After giving the shot, call emergency services right away for transport to the hospitalnhs.uk. Early steroid injection can be life-saving, essentially halting the progression of the crisis in many cases.
- Plan ahead for triggers: Certain high-risk scenarios require planning. For example, before any surgery or invasive dental work, inform the medical team of your Addison’s – you will need IV steroids during the procedure to prevent crisisnhs.uk. For long travel or vacations, pack double your medication plus your injection kit (in case of loss or delays)nhs.uk. Avoid strenuous exercise beyond your usual regimen without discussing stress dosing (extreme exertion can trigger a crisis if you’re not conditioned for it)nhs.uk. It’s also wise to avoid exposure to extreme heat, which can dehydrate you; if you must be in hot weather, stay hydrated and consider a slight increase in salt/fluid intake per your doctor’s advice.
- Treat infections early: Infections are a major trigger for adrenal crisesncbi.nlm.nih.gov. If you suspect an infection (such as pneumonia or a stomach bug), seek medical care early. You may need an antibiotic for bacterial infections, and you absolutely should increase your steroid dose at the first signs of a significant infection (don’t wait for it to get severe)ncbi.nlm.nih.govmy.clevelandclinic.org. For example, even a stomach flu can rapidly cause crisis due to vomiting – in such cases, administer your injection and get to a hospital for IV fluids.
- Medication interactions and other conditions: Some medications can interfere with cortisol metabolism or adrenal function (for instance, rifampin or phenytoin can make you metabolize cortisol faster; etomidate, used in anesthesia, can suppress cortisol; thyroid hormone can “unmask” adrenal insufficiency)ncbi.nlm.nih.govncbi.nlm.nih.gov. Make sure any doctor you see knows you have Addison’s. If you have co-existing conditions like diabetes or thyroid disease (common in autoimmune Addison’s), manage them well – poorly controlled thyroid disease, for example, can precipitate adrenal crises if thyroid medication is started without adequate steroids on boardncbi.nlm.nih.govncbi.nlm.nih.gov.
- Carry identification and educate others: Always wear a medical alert bracelet/necklace stating “Adrenal Insufficiency – needs corticosteroids” and carry a steroid emergency cardnhs.uknhs.uk. In an emergency, this alerts first responders to give life-saving steroids promptly. It’s also wise to inform close friends, caregivers, or coworkers about your condition and emergency plannhs.uk. Teach them how to recognize an adrenal crisis and, if they’re willing, how to give the emergency injection. Having someone around who knows to say “This is an Addison’s crisis – give IV hydrocortisone immediately” when calling 911 can make a huge difference in how quickly you receive proper treatment.
By following these preventive measures, patients can significantly lower their risk of adrenal crisesncbi.nlm.nih.govncbi.nlm.nih.gov. Nonetheless, because not every crisis can be avoided (and we can’t predict every stressor), being prepared to act quickly if one starts is equally important.
Managing an Addisonian Crisis: Immediate Actions and Recovery
Despite best efforts, adrenal crises can still occur – and they require prompt treatment. Here we detail what to do during a crisis and how to promote recovery after the acute phase:
Emergency treatment during a crisis: If an Addison’s patient is in adrenal crisis (or even if you suspect one):
- Administer corticosteroid IM/IV immediately: Time is critical. If you have an emergency hydrocortisone (or dexamethasone) injection kit on hand, use it right away (inject into a muscle)nhs.uk. Don’t worry about giving “too much” – in crisis, high doses are needed, and one timely shot can be life-saving. If no injection is available at home, call emergency services (911) and inform them it’s an “adrenal crisis.” Paramedics typically carry IV hydrocortisone or can be instructed to administer whatever steroid is available en routenhs.uk. Do not wait for definitive diagnostic tests – treatment should be given on the suspicion of crisis, as delays are dangerousncbi.nlm.nih.govncbi.nlm.nih.gov.
- Position and supportive care: While waiting for help, lay the person flat on their back if possible and raise their legs slightly (this helps blood pressure). Keep them warm (since shock can cause body temperature to drop) but not overheated if they have fever – basically maintain a normal body temperature. If they are conscious and able to drink, give them fluids (preferably an oral rehydration solution or sports drink that contains salt and sugar)my.clevelandclinic.org. However, do not give anything by mouth if they are vomiting or extremely drowsy/near-unconscious, due to aspiration risk.
- Monitor vital signs if possible: If you have a blood pressure cuff, pulse, or glucose meter at home, note the readings to relay to EMTs. Often the person will have very low BP, a rapid pulse, and possibly low blood glucose. If blood sugar is low and they are able to swallow safely, a sugary drink or glucose gel can be given while waitingmy.clevelandclinic.org – but again, if they are not fully alert, skip oral intake and wait for IV dextrose from paramedics.
- At the hospital: The standard emergency regimen is IV hydrocortisone (100 mg bolus, followed by doses every 6 hours or a continuous drip) and aggressive IV fluids (normal saline with 5% dextrose is often used to address low blood pressure, low sodium, and low glucose simultaneously)nhs.uk. Blood tests will be run (but treatment starts before results): expect labs for sodium, potassium, glucose, cortisol, ACTH, etc., and possibly an ACTH stimulation test if the diagnosis was not confirmed yet. If infection is a suspected trigger, broad-spectrum antibiotics will be started pending culturesmy.clevelandclinic.org. Supportive care may include oxygen, treatment for hyperkalemia (if potassium is dangerously high), and addressing any other complication like hypoglycemia or arrhythmias. With proper treatment, patients often begin stabilizing within 1–2 hours – blood pressure comes up and mental status improves after steroid administrationncbi.nlm.nih.govncbi.nlm.nih.gov. Close monitoring in an ICU or high-dependency unit might be needed for a day in severe cases.
Recovering from an adrenal crisis: Once the acute crisis is under control (blood pressure stable, patient awake and able to take oral meds), the focus shifts to recovery and preventing recurrence. Recovery can take several days to weeks for one to feel fully “back to baseline.” Here’s what to expect and do:
- Continuation of steroids and taper: Initially after a crisis, the doctor will keep you on higher doses of hydrocortisone for a day or two, then taper down to your normal maintenance dosemy.clevelandclinic.org. For example, they might give IV hydrocortisone for 24-48 hours, then switch to high-dose oral steroids for a couple more days before gradually reducing to your usual dose. This ensures your body is fully “refueled” with cortisol and helps you recover strength. Do not abruptly drop back to your normal dose immediately after a crisis – follow your doctor’s weaning plan.
- Rehydration and diet: Even after IV fluids, you might be somewhat dehydrated or have electrolyte imbalances. Continue drinking plenty of fluids and ensure adequate salt intake as recommended (some patients are told to temporarily increase salt in diet or take salt tablets after a crisis)my.clevelandclinic.orgmy.clevelandclinic.org. Your care team will recheck blood electrolytes to guide this. Eating balanced meals with sufficient carbohydrates is also important to replenish low blood sugar and glycogen stores. If nausea persists, doctors may prescribe antiemetics. Most people get their appetite back as steroids take effect, and weight regained after prior weight loss is a sign of recovery.
- Rest and gradual return to activities: An adrenal crisis is physically akin to a marathon (the body is drained and muscles often break down from cortisol lack). It’s normal to feel extremely tired for several days after. Plan for plenty of rest. Slowly ease back into daily activities – for a 60-year-old, perhaps a few days off work (or lighter duties), help with household chores, etc., until strength returns. Listen to your body; pushing yourself too quickly can delay recovery. Many patients report it takes at least 24-48 hours after treatment just to start feeling somewhat bettermy.clevelandclinic.org, and up to a couple of weeks to fully recover energy.
- Treat the precipitating cause: Ensure that any underlying trigger is addressed to facilitate full recovery. If it was an infection, finish the course of antibiotics and follow up with your doctormy.clevelandclinic.org. If it was due to stopping steroids (in someone who didn’t know they shouldn’t), that will be corrected with education. For other triggers like uncontrolled thyroid disease or severe stress, make sure those are managed (e.g., adjust thyroid medication, seek counseling for emotional stress, etc.). Recovering from a crisis isn’t just about the cortisol – it’s also about not slipping back into one from the same trigger.
- Medical follow-up: After a crisis, schedule a prompt follow-up with your endocrinologist. They may review your maintenance dosing – occasionally, having a crisis signals that your daily dose or fludrocortisone dose might be too low and needs tweaking. They will also reinforce sick-day rules and may adjust your emergency plan. It’s a good time to renew or obtain any supplies you used (get a new emergency injection kit if you used yours).
- Monitor yourself: In the weeks following a crisis, be vigilant about any lingering or returning symptoms. Check your blood pressure if you have a home cuff, and report if it’s consistently lower or higher than your usual (too low might mean you need a bit more fludrocortisone; too high could mean you’re on a bit too much). Also watch for swelling (if fludrocortisone was increased) or signs of over-replacement like difficulty sleeping or weight gain, and discuss with your doctor. Keeping a symptom diary can help you and your doctor fine-tune your treatment after a crisis.
- Support your body: General healthy practices aid recovery – ensure you get enough sleep, maintain a consistent daily schedule for your meds, and avoid additional stress if possible until fully recovered. Gentle exercise can be resumed once you’re feeling stronger, but don’t push to high-intensity workouts right away.
Most people survive adrenal crises if treated in time, and they can return to their normal health with appropriate recovery caremy.clevelandclinic.orgmy.clevelandclinic.org. However, an adrenal crisis is a serious event; having one may be psychologically distressing. Some patients benefit from speaking with a counselor or joining Addison’s support groups to discuss the experience and anxiety around it. Importantly, having had a crisis once means you must be even more vigilant: studies show those who have had one crisis are at higher risk of another if precautions aren’t strictly followedncbi.nlm.nih.gov. But by learning from it – adjusting medication doses during stress more aggressively, for instance – you can hopefully prevent future emergencies.
Factors That Can Worsen an Adrenal Crisis Severity
An Addisonian crisis is by definition life-threatening, but certain factors can make a crisis even more severe or harder to treat, increasing the risk of complications or death. These include:
- Delay in treatment: The longer a person in crisis goes without receiving cortisol replacement, the more profound the shock and metabolic disturbances becomencbi.nlm.nih.gov. Delayed treatment is a major factor that makes an adrenal crisis more likely to be fatalncbi.nlm.nih.gov. For example, if someone collapses and the diagnosis is missed for hours, or if a patient hesitates to use their injection, the patient may progress to cardiac arrest from hypotension. Timely injection within the first hour or two of crisis onset can literally be the difference between life and deathncbi.nlm.nih.govncbi.nlm.nih.gov.
- Severe infection (sepsis): If a crisis is precipitated by a severe infection, such as sepsis from pneumonia or abdominal infection, the patient’s body is dealing with two shocks at once (septic shock + adrenal shock). Infections like meningococcal disease can cause adrenal bleeding (Waterhouse-Friderichsen syndrome) leading to a catastrophic crisis that is notoriously fatal if not immediately treated. In Addison’s patients, even a moderate infection can rapidly escalate adrenal insufficiency. Crises triggered by gastroenteritis (vomiting/diarrhea) are also particularly dangerous because the patient can’t retain oral meds – dehydration and electrolyte derangements happen quickerncbi.nlm.nih.govncbi.nlm.nih.gov. In any infection-triggered crisis, prompt steroid and appropriate antimicrobials are needed; untreated or very severe infections make the crisis harder to reversencbi.nlm.nih.govmy.clevelandclinic.org.
- Cardiovascular disease or frailty: In a 60-year-old (or any older adult) with underlying heart disease or frailty, an adrenal crisis can be more life-threatening. Low cortisol amplifies hypotension and can precipitate cardiac arrhythmias (especially with high potassium), which an older heart may not tolerate. Indeed, advanced age and comorbidities are recognized risk factors for worse outcomes in adrenal crisesncbi.nlm.nih.gov. An older patient is more likely to experience organ failure during a crisis due to limited physiological reservesthelancet.com. For instance, an elderly Addison’s patient might suffer an acute kidney injury during crisis more readily than a younger person.
- Hyperkalemia and hypoglycemia: Adrenal crises often involve high potassium and low glucose due to aldosterone and cortisol deficiency. Very high potassium levels can cause dangerous heart rhythm disturbances (even cardiac arrest), and very low blood sugar can lead to seizures or brain injurymy.clevelandclinic.orgmy.clevelandclinic.org. If a crisis presents with extreme hyperkalemia (from prolonged aldosterone lack) or severe hypoglycemia (more common in children but possible in adults with poor intake), the immediate danger is heightened. Such patients need urgent interventions (calcium, insulin/glucose for hyperkalemia; IV dextrose for hypoglycemia) in addition to hydrocortisone. Delays or inadequacy in correcting these can make the crisis more lethal.
- Concurrent adrenal damage or hemorrhage: Occasionally, an adrenal crisis is compounded by an acute event like bilateral adrenal hemorrhage (for example, in someone on blood thinners or with trauma). This means the adrenal glands acutely lose all function at once. These crises can be very severe and often come with other issues like disseminated intravascular coagulation if due to sepsis. They might present with additional symptoms like flank pain (from bleeding into the gland) and tend to be rapidly fatal without aggressive care.
- Inadequate dosing or undertreatment: If, during a crisis, the steroid dosing or fluids given are not sufficient (for instance, if a patient is inadvertently given too low a dose of hydrocortisone or if their IV fluids don’t contain dextrose when needed), the crisis may not improve and can worsen. Guidelines indicate that blood pressure should start rising within 1 hour of proper therapyncbi.nlm.nih.gov; if not, it signals that either the treatment is inadequate or there’s another compounding issue (like ongoing bleeding or cardiac issue).
- Polyendocrine crises: Some Addison’s patients have other endocrine disorders (like type 1 diabetes or hypothyroidism). If a diabetic Addison’s patient has very low blood sugar from crisis and is dealing with insulin management, or if a person with hypothyroidism doesn’t have enough thyroid hormone during a crisis, it can complicate and worsen the situation. For example, untreated hypothyroidism during adrenal crisis can make it harder to raise blood pressure (myxedema-adrenal coma overlap). Patients with polyglandular autoimmune syndrome need careful management of all conditions during stressncbi.nlm.nih.gov.
- Lack of awareness or misdiagnosis: Sometimes an adrenal crisis is made more dangerous if medical personnel fail to recognize it. If a patient is brought to a small emergency department and staff attribute symptoms to something else (say, a stomach flu or heart failure) and don’t give steroids promptly, the patient’s condition can deteriorate quickly. Ensuring that Addison’s patients carry emergency info (cards/bracelets) and that paramedics/hospitals follow emergency guidelines is crucial to avoid this scenarionhs.uknhs.uk.
Bottom line: Any adrenal crisis is serious, but an older patient or one with other health issues has less “cushion.” For a 60-year-old woman with Addison’s, crises can indeed be more dangerous than in a young person, so prevention and rapid treatment are paramount. Studies have shown that even with optimal care, there is still an estimated mortality of around 6% in known adrenal insufficiency patients who experience crisisncbi.nlm.nih.gov – emphasizing how critical it is to manage these factors. Fortunately, by anticipating these issues (for example, increasing steroids early in an infection, or closely monitoring an older patient’s heart during a crisis), healthcare providers can mitigate some of the risk.
